Digital Twins on Jinkō
Table of Contents
- Executive Summary
- Nova's Digital Twin Solution High Level
- Science And Methodology
- Jinkō the Technology Behind It
- Use Cases
- Treatment De-escalation
- Long-Term Clinical Outcomes Prediction for Market Access - ASCVD (Inclisiran)
- Hematological Malignancies - Drug Development Support
- Patient Population Selection - Acute Myeloid Leukemia (AML)
- Trial Design & Efficiency - Atopic Dermatitis (AD)
- Dose-Response Modeling - T-cell Engager
- Adverse Effects - Neutropenia
- Data Integration in Drug Development - Best Responders Identification
- Synthetic Control Arm for Rare Diseases
- EGFR-TKI Treatment Combination - NSCLC
- Treatment Combination - Chronic Hepatitis B (HBV)
- Transposability Study - Population Extrapolation
- Trial Rescue/Monitoring - Subcutaneous to IV Administration
- Treatment Regimen Optimization
- Tangible Benefits of Digital Twins for Drug Developers
- How we partner
- Nova In Silico: Company Description and Credentials
Executive Summary
Nova In Silico is a pioneer in digital twin (DT) technology for clinical research, offering a proven platform that simulates patient outcomes with high fidelity. The flagship Jinkō platform integrates mechanistic disease modeling with AI/ML algorithms to create virtual patient “twins” and entire in silico cohorts (virtual populations) that mirror real patients’ characteristics and treatment responses. This approach has been validated in oncology and beyond, with a notable success in accurately predicting the results of a Phase III lung cancer trial (FLAURA2) within hours, closely matching the real outcome prospectively.
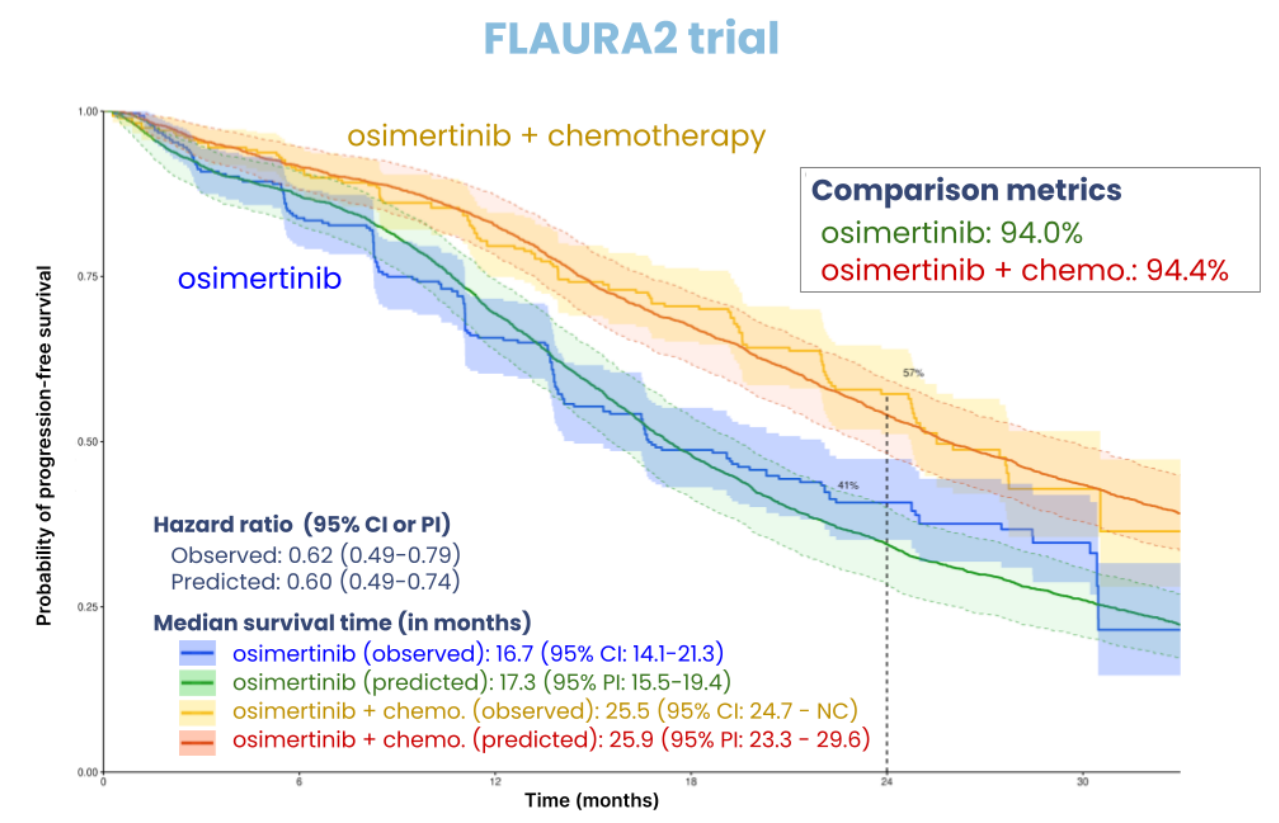
Kaplan-Meier curves of observed PFS and simulated TTP for FLAURA2 trial (both arms).
The comparison metrics is the percentage of non-significant bootstrapped weighted log-rank tests (predicted vs observed data)
Nova's DT solutions aim to deliver several benefits to drug developers, including better trial design and success rates by optimizing protocols and identifying best-responders, efficiency and cost savings through reduced sample sizes and trial durations, patient-centric insights by exploring rare populations and biomarkers, and regulatory alignment through transparent and traceable white-box modeling. The company emphasizes a service-based collaboration model, leveraging a team of over 40 experts (scientists, engineers, biologists, clinicians, and medical doctors) and an extensive library of over 100 disease and treatment models.
The Jinkō platform is designed for full transparency and auditability, streamlined workflow, and efficient collaboration. It supports model building and training, clinical trial simulation, calibration, results display and analysis, and documentation. The platform also incorporates AI/LLM tools to accelerate model development, data extraction, and processing, and to facilitate interaction with non-modeling specialists. Nova's methodology is rooted in Quantitative Systems Pharmacology (QSP) models, which are built on a causal and mechanistic understanding of disease progression and drug action, making them less data-hungry and more interpretable than traditional AI approaches.
Nova's Digital Twin Solution at a High Level
Nova’s Digital Twin solution is built on Jinkō, an enterprise-grade AI platform purpose-built for biopharma. This solution constructs synthetic cohorts by integrating preclinical and clinical data from multiple sources and modeling individual patient trajectories using causal models calibrated via machine learning algorithms on real-world data. The core components and features of Nova's Digital Twin solution include:
-
Jinkō Platform: A robust clinical trial simulation platform that creates virtual patients and cohorts to predict clinical outcomes. It integrates mechanistic disease modeling with advanced AI/ML for data integration, model training, and validation.
-
Knowledge Management Module: Empowers users to collect, curate, and share scientific insights directly within the platform. It allows uploading references, extracting pertinent information, and annotating key findings, ensuring centralized and accessible knowledge. These insights are linked to modeling and simulation projects for transparency and traceability.
-
Virtual Patient Engine: Generates virtual patients by leveraging prior knowledge and real-world data from various sources (clinical trials, real-world evidence, molecular profiles, biomarkers, preclinical data). Each virtual patient is a high-fidelity construct with demographic, disease-specific, and biomarker attributes. The system can generate an unlimited number of virtual patients to capture population variability, including rare subpopulations.
-
Mechanistic Disease and Treatment Models: Unlike purely statistical twins, Nova’s digital twins are grounded in biophysical and pharmacological models. These models describe disease progression (e.g., tumor growth kinetics, immune response) and drug mechanisms of action (PK/PD relationships) in mathematical terms. They are calibrated using available data to reproduce known outcomes and variability.
-
AI-Powered Calibration & Prediction: Utilizes AI/ML techniques for parameter fitting and predictive power improvement. Algorithms like Bayesian optimization and machine learning ensure virtual cohort outcomes match real-world patient outcomes. The system trains digital twin models to reliably predict individual patient trajectories, generating synthetic control arm predictions for trial forecasting.
-
End-to-End Trial Simulation Workflow: Jinkō provides a comprehensive solution from data ingestion to simulation output. The workflow includes data integration and cleaning, model development (adapting disease models to trial context), model validation (verifying against known data), and large-scale simulations of virtual patients through trial protocols. It enables rapid in silico simulation of entire Phase 1 to 4 trials.
-
Output & Decision Support: The solution provides comprehensive trial-outcome predictions (e.g., virtual PFS curves, response rates, dose-response curves) with uncertainty measures. An integrated analytics suite offers interactive visualizations and supports data overlays to compare simulated results against observed clinical data. This framework ensures auditability and interpretability for decision-making and regulatory submissions.
Science And Methodology
Nova In Silico's scientific methodology is fundamentally rooted in Quantitative Systems Pharmacology (QSP) models, which provide a mechanistic and causal understanding of disease progression and drug action. This approach is complemented by advanced AI/ML techniques to enhance efficiency, scalability, and interpretability. The core principles and methodologies are:
-
Quantitative Systems Pharmacology (QSP): Nova builds in silico clinical trials, including synthetic control arms (SCAs) and digital twins, using QSP models. These models are based on a causal and mechanistic understanding of disease progression, drug mechanisms of action, and physiological sources of intra- and inter-patient variability. This knowledge-driven approach is transparent, making models and results easily interpretable, and requires less data compared to traditional AI approaches.
-
Three Pillars of QSP Models:
- Disease Model: A mechanistic model simulating biological pathways and processes to predict disease progression.
- Drug Model: Pharmacokinetic models simulating how drugs behave in the body.
- Virtual Population (Vpop): Virtual populations simulate patient variability by using values from disease model parameters, capturing both inter- and intra-patient differences.
-
Patient-Level Digital Twins vs. Population-Level Approach: Nova's methodology supports both:
- Population-level approach: Aims to create a cohort of virtual patients that shares the same baseline distributions as the target population, without necessarily matching each individual patient's characteristics to an individual virtual patient.
- Patient-level approach (digital twin): Aims to match one virtual patient’s baseline characteristics to the baseline characteristics of an individual patient in the target cohort, thus creating digital twins for each patient. This allows for simulating how the same patient might fare under different treatments.
-
Addressing Limitations of Traditional Methods: Nova's QSP-based SCAs aim to overcome limitations of other AI-driven SCA approaches by:
- Less data dependency: QSP models require high-quality data but are not as data-hungry as typical AI models, often leveraging summary data.
- Reduced bias and confounding: Mechanistic knowledge in comprehensive QSP models allows for better representation of hidden biological factors, supporting the generation of digital twins that closely match the actual clinical trial population. Causal modeling enables more reliable extrapolation.
- "White box" approach: QSP models are built on knowledge of the target disease’s pathophysiology, providing a transparent understanding of how input data and model parameters influence outputs, fostering confidence in their validity.
| Feature | Traditional External Control Arms (ECA) | AI-Driven SCA — Traditional AI approaches | AI-Driven SCA — Nova’s SCA |
|---|---|---|---|
| Methodology | Statistical matching (propensity score) | Machine learning | Transparent QSP model + digital twins |
| Data Source | Historical clinical trials, RWD | Same + omics & pre-clinical | Same data but can work when data are sparse |
| Strengths | Ethical, quick, low-cost | Improved patient matching, personalised sims, handles big data | Improved patient matching, personalized simulation with fewer and heterogeneous data, lower bias, white box approach with easy what-if testing |
| Weaknesses | Hidden bias, data mismatch | Data-hungry, black-box, bias risk | Needs a good understanding of the pathophysiology of interest |
| Regulatory Acceptance | Increasing but with scrutiny | Emerging, needs proof | Emerging but easier to justify due to explainability |
-
In Silico Clinical Trial Methodology and Framework:
- Study Design: Each virtual patient can serve as its own control, duplicated and simultaneously assigned to all treatment arms. In silico trials are conducted on large virtual populations representative of the population of interest, with no limitation on the number of virtual patients.
- Efficacy Measurement: Efficacy is determined at the individual level by directly comparing outcomes under investigational treatment vs. control for each virtual patient. It is free from inter-patient variability between treatment arms, sampling fluctuations, and bias from external factors or loss to follow-up, as the simulation environment is perfectly controlled.
- Interpretation of Results and Uncertainty Management: Efficacy is reported with a 95% predicted percentile interval (95% PPI), measuring prediction uncertainty including model uncertainties and inter-patient variability. It is calculated using a bootstrap approach with a sample size matching a comparable real-world RCT. There are no issues with statistical power, and no limitation on endpoints, comparators, or subgroup analyses.
-
Model Validation: Nova validates its models for predictive accuracy and reliability through:
- Internal checks: Continuous structural validation of model design, hypotheses, code-base consistency, and sanity checks.
- Retrospective validation: Comparison of model simulation results to data not used during the training phase (e.g., training/validation data split or different studies for training and validation), as demonstrated in recent scientific publications.
- Prospective validation: Comparison of model simulation results to data not available at the time of output production, as demonstrated by the successful prediction of FLAURA2 Phase III clinical trial outcomes.
Nova's methodology allows for the integration of heterogeneous data sources (in vitro, preclinical, clinical, real-world data) and supports complex treatment histories. It can model treatment outcomes for current standard of care and simulate different treatment regimens, integrating relevant efficacy clinical trial endpoints like overall survival (OS), objective response rate (ORR), and progression-free survival (PFS).
Jinkō - The Technology supporting the science
Jinkō is Nova In Silico's flagship enterprise-grade AI platform, purpose-built for biopharma. It serves as the central hub for Nova's digital twin solutions, streamlining the entire clinical trial simulation and design optimization process. Jinkō combines robust scientific modeling with AI and software engineering practices to provide a comprehensive, efficient, and transparent platform for in silico clinical trial simulation, accelerating drug development and enabling better decision-making. Key technological aspects and features of Jinkō include:
-
Integrated Platform: Jinkō offers multiple functions within a single platform, supporting modeling, simulation, calibration, results display and analysis, and documentation. It ensures full transparency, auditability, efficient collaboration, and a streamlined workflow.
-
AI/LLM Integration: Jinkō incorporates advanced AI and Large Language Model (LLM) tools to accelerate various stages of the workflow:
- Automated Model Generation: AI agents can read and interpret scientific publications, extracting LaTeX-formatted equations and parameter data to automatically generate computational models. This significantly reduces the time required to implement models from literature amd reduce reproducibility issues. Since rolling out the "Paper-To-Model" feature, more than 50% of the models imported in our model library have been generated with the help of Kōhai with a time savings of roughly 60% versus building the model by hand.
- Data Extraction and Wrangling: AI agents parse content from data tables in scientific papers, acquire and format data, and generate code transformations to adhere to expected schemas, fast-tracking data manipulation for calibration and validation.
- Parameter Estimation: AI algorithms are used for estimating unknown model parameters (model calibration) through step-wise approaches like the CMAES algorithm. The estimated parameters represent plausible biological variables or phenomena.
- Conversational Agent (Kōhai): Kōhai acts as a powerful agent and diligent assistant, enabling non-modeling experts to interact with the platform using natural language. It can build models from publications, drag and drop existing models, get experiment summaries, and interpret models and data repositories.
-
Computational Efficiency: Jinkō is designed for high numerical efficiency, leveraging Just-in-Time (JIT) compilation, parallelization of large-scale virtual patient populations, and adaptive, implicit solvers for Ordinary Differential Equations (ODEs). This optimizes execution speed and enables rapid analysis of results, even with millions of virtual patients.
-
Interoperability and Integration: Jinkō supports model interoperability and workflow integration through:
- Parsers and Exporters: Dedicated parsers and exporters for widely used tools like Monolix, SimBiology and Julia, as well as open standards like SBML. This facilitates model exchange and integration across various computational environments.
- Comprehensive API: An extensible API allows programmatic interaction with every component of the model, including structural equations, parameter definitions, and trial designs. This supports automation, external pipeline integration, and fine-grained model editing.
- Python SDK and Cookbooks: Supplemented by a Python SDK and curated examples to help users integrate Jinkō into existing workflows.
-
Model Library: Jinkō hosts an extensive library of over 100 validated disease and treatment models, including internally trained/validated models and curated imports. This library covers various therapeutic areas, providing a head-start for new projects.
-
Traceability and Auditability: All modeling components (models, virtual populations, simulation protocols, supporting documents) are version-controlled, enabling complete traceability of model evolution. Linked assumptions, data, and documentation provide transparency for internal review and external inspection.
Use Cases
Nova In Silico has a strong track record of applying digital twins across various therapeutic areas and clinical development phases. The following are illustrative use cases demonstrating the application of Nova’s digital twin technology and the Jinkō platform:
Non-Small Cell Lung Cancer (NSCLC) Treatment De-escalation
- Context: The objective was to identify the best pemetrexed maintenance de-escalation strategies in FLAURA2 regimen as front-line treatment of metastatic EGFR-mutated non-small cell lung cancer (NSCLC) that would preserve clinical efficacy while reducing treatment intensity. This involved the creation of digital twins-based in silico clinical trials simulating both historical and synthetic alternative arms of the FLAURA2 Phase III clinical trial.
- Methodology: Nova leveraged a previously validated NSCLC QSP model, drug models for osimertinib, platinum-based chemotherapy, and pemetrexed, and a digital-twin cohort from the FLAURA2 trial. They generated synthetic treatment arms for 20+ de-escalation strategies and ran simulations to compare their clinical efficacy with historical trial arms, using each virtual patient as their own control.
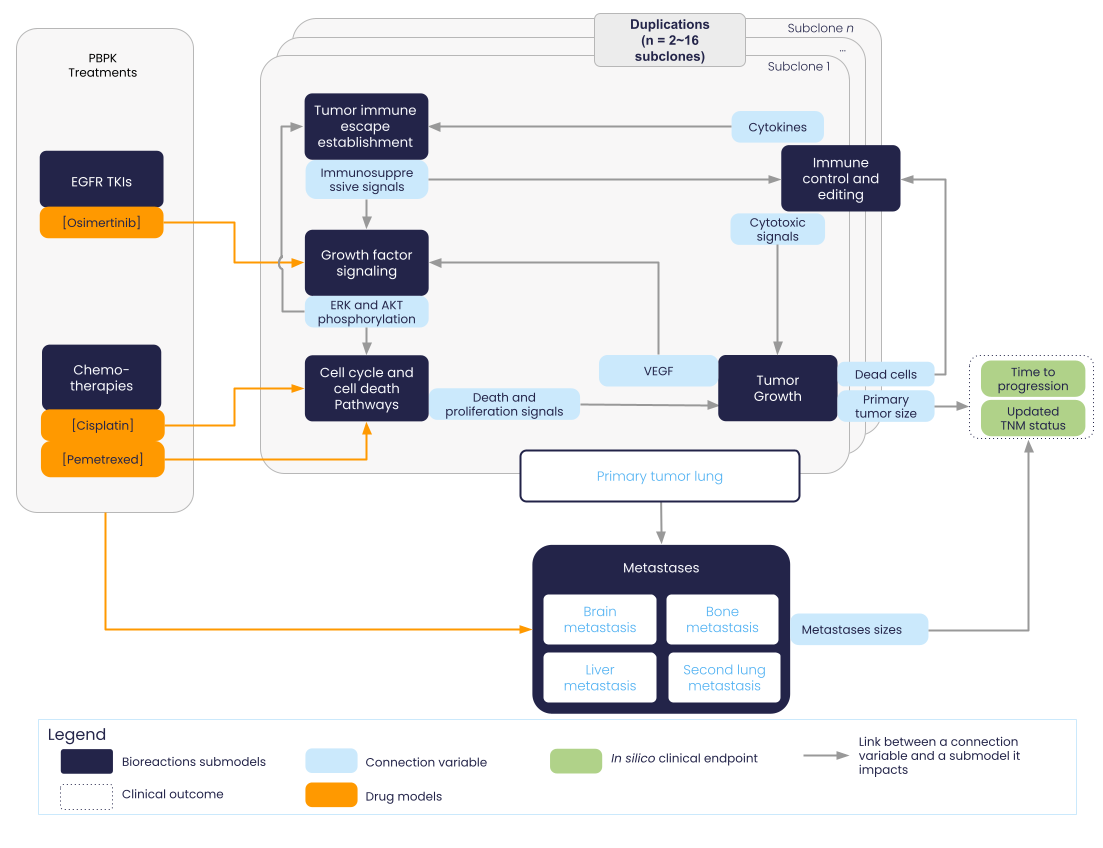
Nova NSCLC model structure.
- Results: Presented at ESMO congress (october 2025), the simulations results identified the best de-escalation strategy. Performing an equivalent study with in vivo clinical trials would have required the enrollment of 11,120 patients and taken over 36 months. In contrast, using the existing in silico model, the study was completed in just 2 months, demonstrating rapid exploration of treatment optimization scenarios.
Long-Term Clinical Outcomes Prediction for Market Access - ASCVD (Inclisiran)
- Context: Nova’s atherosclerotic cardiovascular disease (ASCVD) model was built to predict the 5-year comparative effectiveness of inclisiran versus placebo or active comparators on major cardiovascular events (MACE) for market access purposes.
- Inclisiran is a small interfering RNA (siRNA) therapy targeting PCSK9 mRNA, administered twice-yearly
- It produces substantial and sustained reductions in LDL-C in patients with ASCVD
- However, its long-term effects on cardiovascular outcomes have yet to be established
- Demonstrating cardiovascular benefits with lipid-lowering therapy typically requires large, long-duration randomized clinical trials.
- Methodology:
- Step 1: QSP/mechanistic model of ASCVD
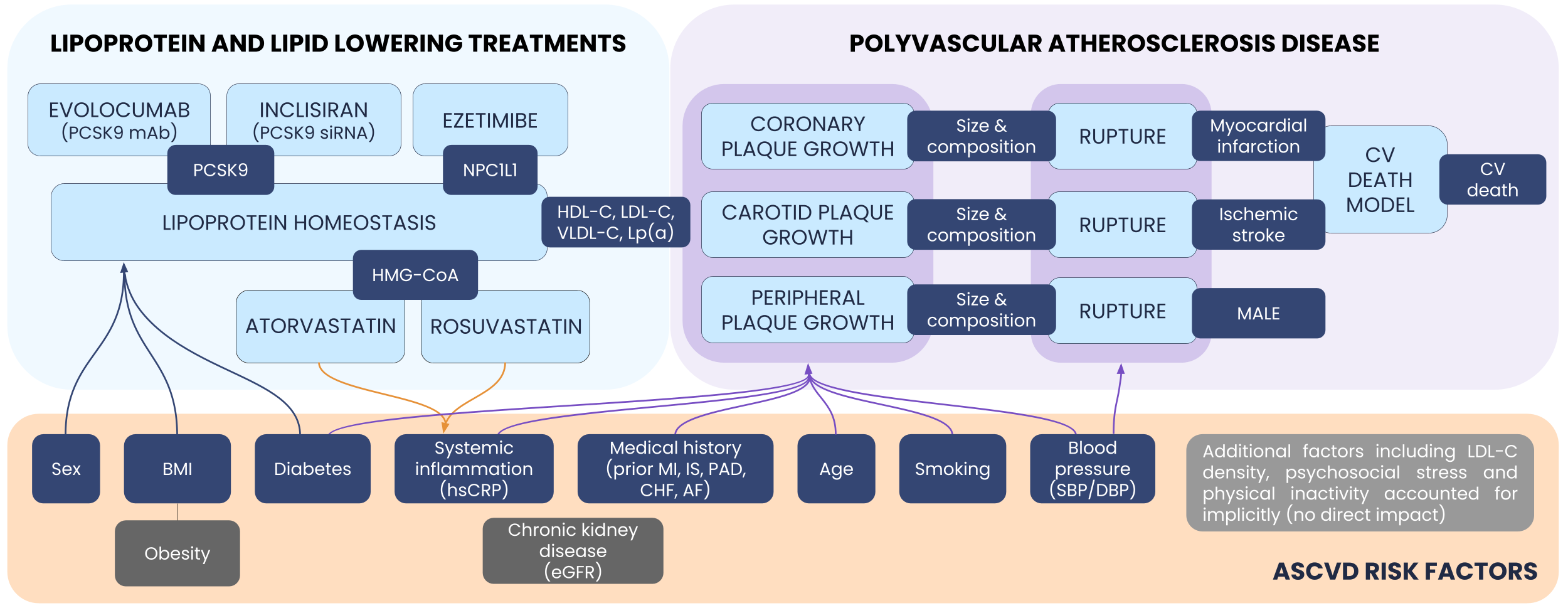
Nova ASCVD model structure.
- Step 2: Calibration and validation. The model has been calibrated (using ORION-10 and FOURIER data), and validated (using ORION-11, FOURIER-OLE, and ODYSSEY OUTCOMES data). This enabled generation of various synthetic arms, including background therapy (statin +/- ezetimibe) + placebo, background therapy + active comparators (ezetimibe, evolocumab, alirocumab), and background therapy + investigational treatment (inclisiran).
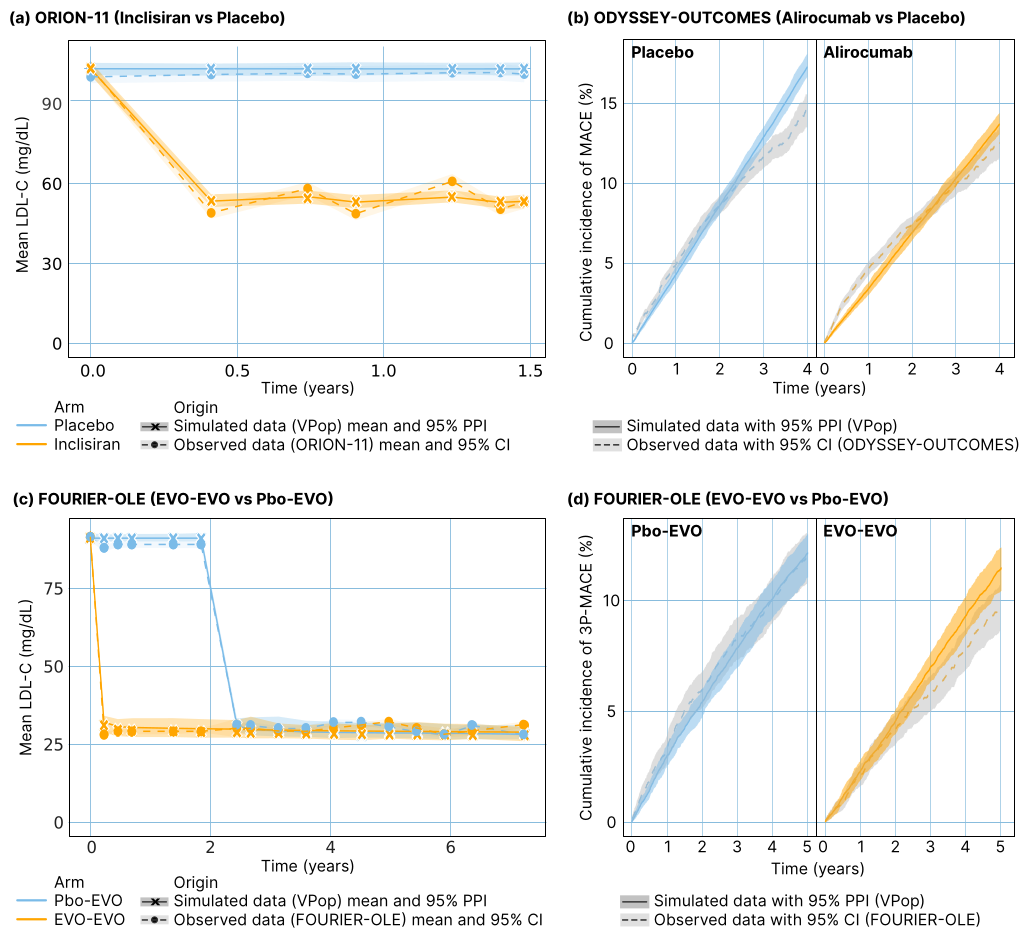
Main validation results on LDL-C and MACE.
-
Step 3: In silico trial simulation. The SIRIUS in silico trial (NCT05974345) was conducted by applying the model to a virtual population with established ASCVD
-
Results: The in silico trial provided early insights into inclisiran’s potential effect on CV events, suggesting a substantial 3P-MACE reduction several years before ongoing Phase III trial results (ORION-4, VICTORION-2-Prevent) would be available. Simulation results were included in a dossier submitted to the French regulatory agency (HAS). This was the first evaluation of an in silico trial by the HAS, and the results were considered exploratory. The work has been presented at international congresses and published (Angoulvant et al., Eur J Prev Cardiol. 2024; Wang et al., NPJ Digit Med. 2025; Angoulvant et al., Poster EAS 2024).
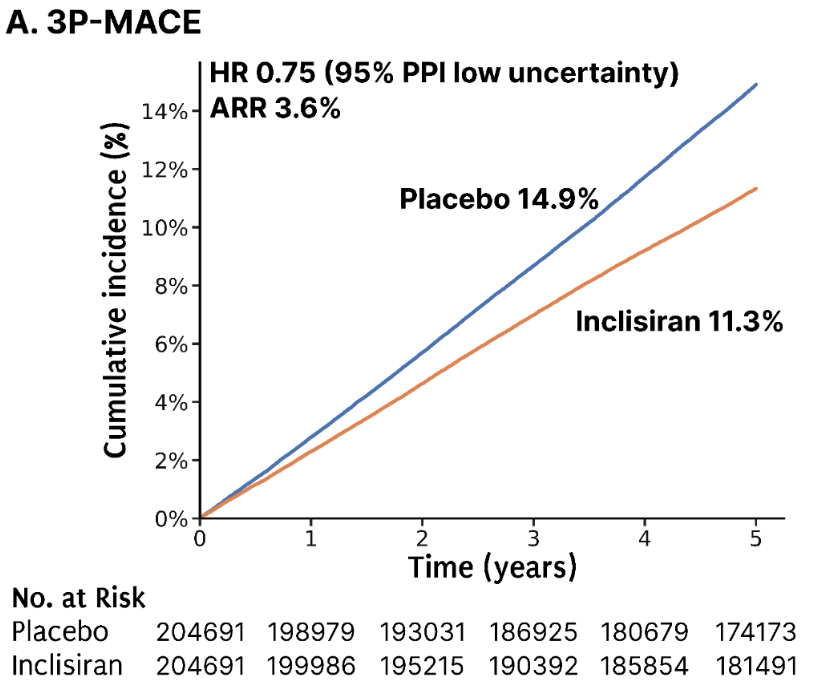
Cumulative incidence of 3P-MACE in SIRIUS trial with inclisiran (orange) vs placebo (blue) in add-on of HI statin +/- ezetimibe (N=204,691).
Hematological Malignancies - Drug Development Support
- Context: Nova continuously develops a QSP platform to support drug development in hematological malignancies, including preclinical to FIH (First-in-Human) translation and Phase 2 & 3 studies.
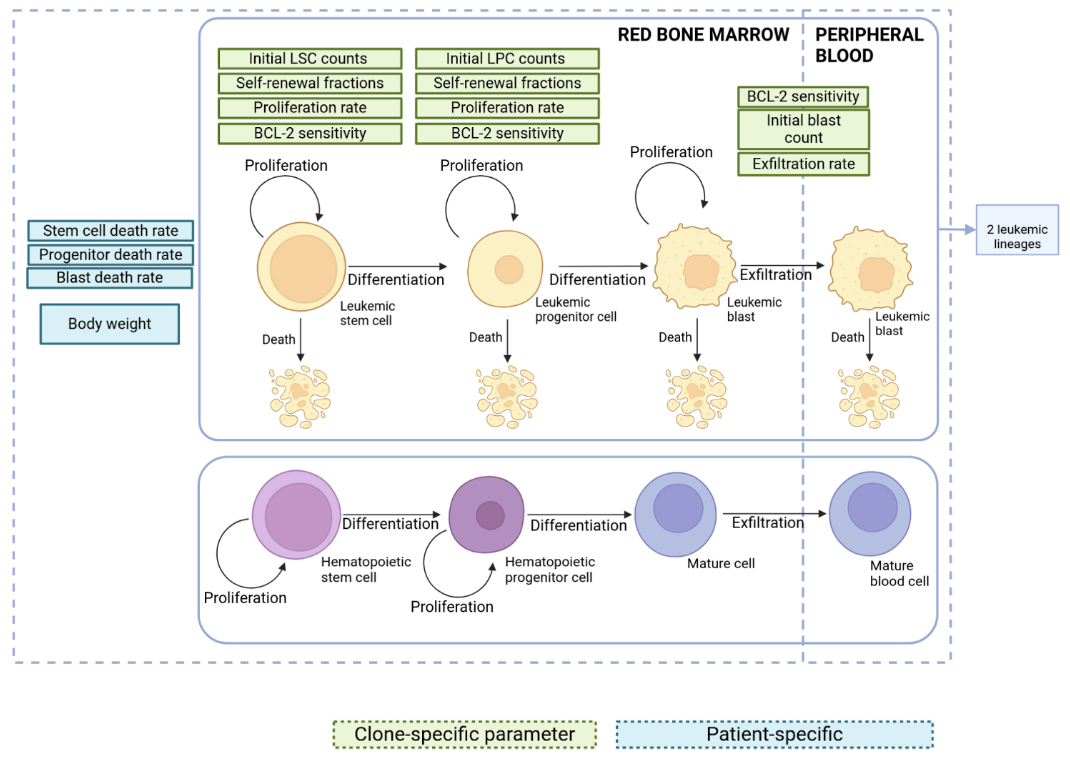
Nova AML model graph
- Methodology: The platform supports indications like AML, CHL, and B-cell and T-cell nHL. It can be combined with various treatment models (T-cell engagers, ADCs, mAbs) and used notably to produce synthetic control arms for existing standards of care (e.g., R-squared, Venetoclax, Azacitidine).
- Results: The platform has been used to investigate various modalities, including potential synergies between new treatment and standard of care in early clinical development. An example use case involved calibration and validation on publicly available data for an ADC, presented at ACOP 2024 (poster).
Patient Population Selection - Acute Myeloid Leukemia (AML)
- Context: To improve outcomes in AML, understanding response variability to the standard Venetoclax + Azacitidine (VEN-AZA) therapy is essential.
- Methodology: Nova built a model that mechanistically integrates the pharmacokinetics as well as the mechanisms of action of VEN and AZA.
- Results: The model successfully reproduces observed responses in both in vitro settings and clinical trials, including blast count reductions and changes in white blood cell counts. Analyses show that patients with higher MAC scores (a measure accounting for BCL-2 levels relative to MCL-1 and BCL-xL on leukemic cells) tend to respond better to VEN-AZA therapy, suggesting that baseline anti-apoptotic protein expression is predictive of efficacy. A poster was presented at AcoP.
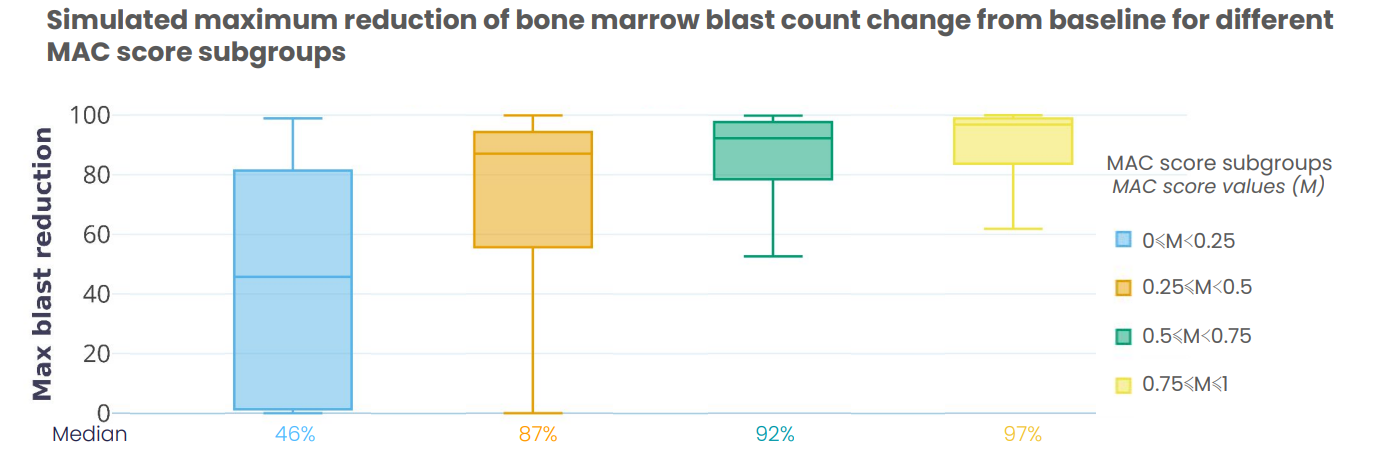
Trial results comparing maximum reduction of bone marrow blast count change from baseline for different MAC score subgroups after Ven + Aza treatment. MAC Score represents the ratio of Bcl-2 expression over other anti-apoptotic protein expression (BCL-xL and MCL)
Trial Design & Efficiency - Atopic Dermatitis (AD)
- Context: High phenotypic diversity in Atopic Dermatitis leads to high diversity of treatment response. The goal was to evaluate biomarker-based inclusion strategies to optimize trial design.
- Methodology: Nova developed a QSP model and a virtual population representing the phenotypic diversity of AD to generate synthetic control and interventional arms. The resulting virtual population was analyzed to identify predicted best responders, generating hypotheses for optimal biomarker-based inclusion strategies.
- Results: The study predicted a minimal set of 4 markers that explain most of the response to treatment, leading to a predicted 25% improvement in screened patient numbers for biomarker-based inclusion strategies.
Dose-Response Modeling - T-cell Engager
- Context: In the context of developing a bispecific antibody in combination with a standard of care for lymphoma patients, the sponsor had to proceed with a dosing adjustment for an ongoing Ph. 3.
- Methodology: Nova built a QSP model of T-cell engager synapse formation and cytotoxicity. This mechanistic approach allowed for calibration using in vitro data and translation to human predictions when combined with a PBPK model and disease model. A virtual population was calibrated using subsampling to reproduce the aggregated data of 3 different clinical studies.
- Results: The final model was used to support dose selection for a Phase 3 trial, with respect to tumor reduction and tumor progression endpoints. Specific results are not yet publicly disclosed.
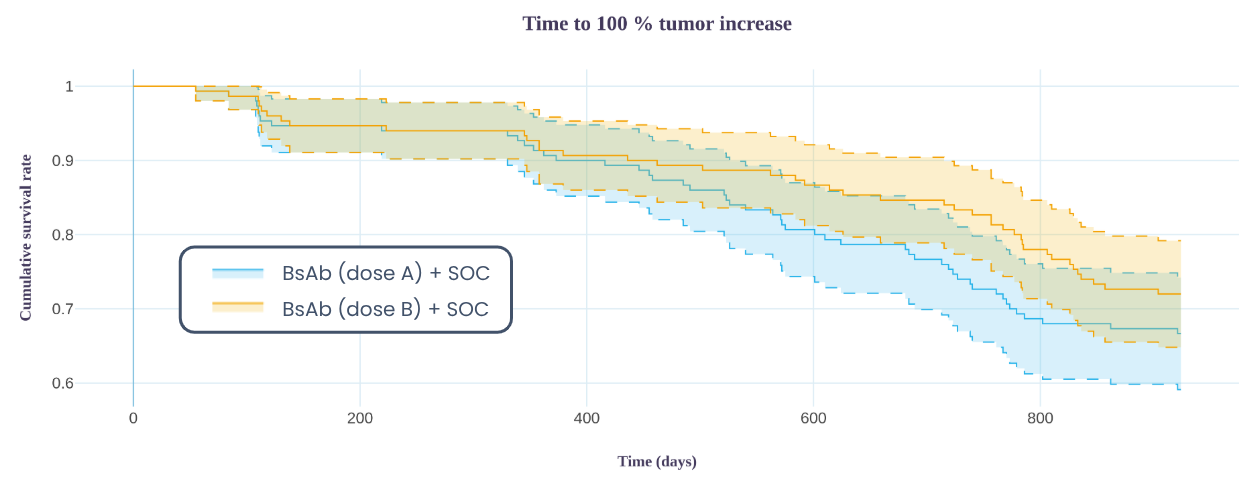
Trial results of time to 100% tumor increase above nadir (proxy for progression-free survival), comparing two BsAb doses in combination with the SOC
Adverse Effects - Neutropenia
- Context: A sponsor was developing a treatment with potential blood toxicity (neutropenia) and postulated that an alternative drug regimen could minimize adverse effects while maintaining efficacy. They had Phase 2 adverse effects data with various doses.
- Methodology:
- A computational model of treatment-induced neutropenia was developed, by adapting the model propoposed by Cho et al. (2018). Our model was informed by the sponsor’s Phase 2 data.
- Simulations were run on a virtual population with three regimens (R1, R2, R3) having different area under the curve (AUC) and maximun plasma concetration (Cmax) profiles.
- The predicted minimum neutrophil numbers in blood were compared.
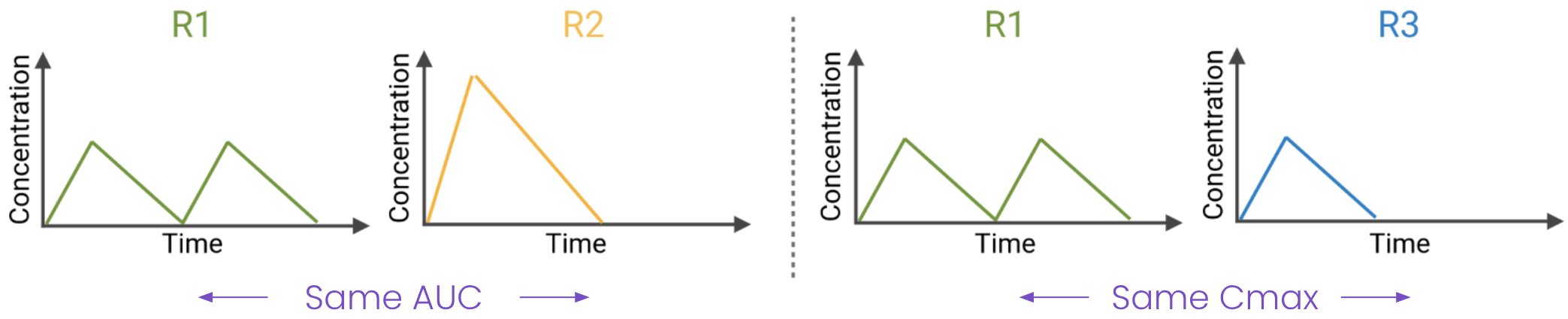
Illustration of the pharmacokinetics profile of the different regimens. AUC: area under the curve; R[1-3]: Regimen [1-3]; Cmax: maximum plasma conctration.
- Results: The model predicted that AUC (total exposure) is the main driver of neutropenia, suggesting that accumulation of damage on neutrophil progenitors scales with total exposure rather than acute toxicity. Regimen R3 was favored to reduce adverse effects, with further simulations to verify efficacy maintenance.
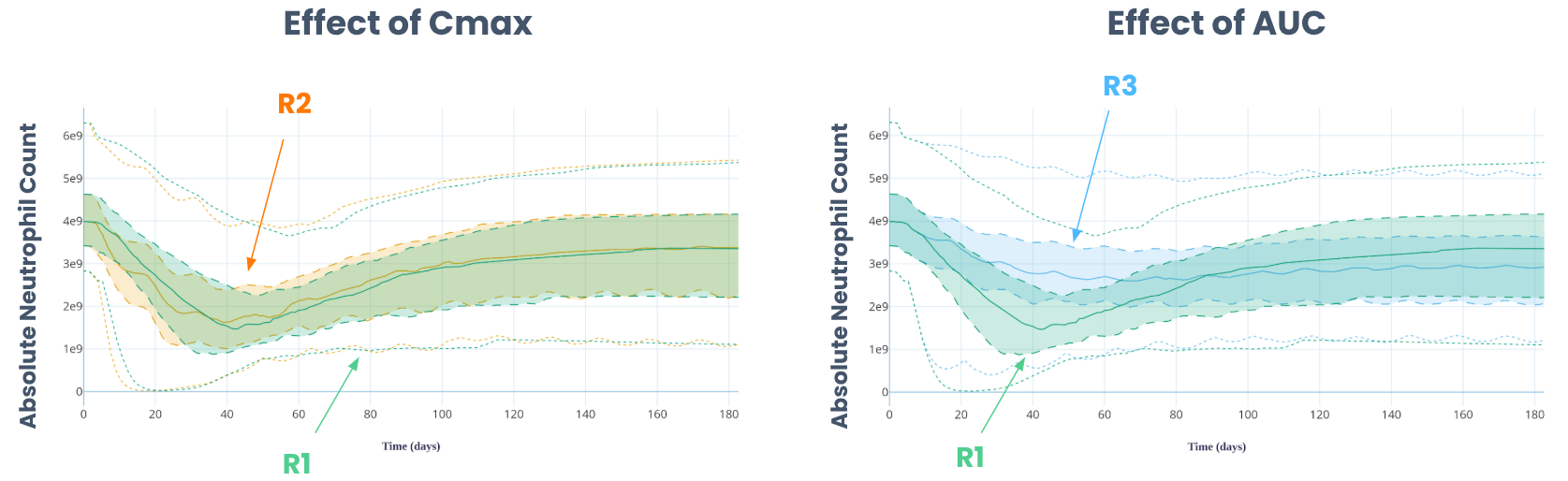
Effect of Cmax and AUC on absolute neutrophil counts. AUC: area under the curve; R[1-3]: Regimen [1-3]; Cmax: maximum plasma conctration.
Data Integration in Drug Development - Best Responders Identification
- Context: A sponsor wished to launch a Phase III clinical trial on patients most likely to respond to an investigational treatment, but existing data was heterogeneous across preclinical and clinical sources.
- Methodology: A comprehensive mechanistic modeling approach was developed to integrate data from preclinical to early clinical stages. The model was leveraged to inform Phase III trial design and outcomes, specifically to determine characteristics of best responders.
- Results: The approach led to the identification of best responders, defined as patients with PFS at least 6 months higher in the investigational arm than in the standard of care arm. Key characteristics impacting response (e.g., specific mutations, initial cancer stage, depth of proliferating layer) were identified, allowing for adaptation of inclusion/exclusion criteria.
Synthetic Control Arm for Rare Diseases
- Context: Recruitment for rare disease Phase III trials is exceptionally difficult due to patient scarcity and ethical constraints on control arms, often forcing the use of suboptimal designs that compromise statistical power and increase regulatory risk.
- Suboptimal designs: sponsors are compelled to use smaller-than-typical populations and implement statistically limited trials (e.g., single-arm studies or adaptive designs without full randomization) to meet minimal enrollment goals. (Getz, 2025 ; Bell et. al, 2014)
- Ethical Challenge: the need for randomization forces the assignment of scarce patients to a potentially less effective Standard of Care (SOC), exacerbating the risk in a trial less likely to produce definitive efficacy data
- Methodology: Synthetic additional control arms (SCAs) can be generated using an appropriate mechanistic model calibrated and validated on data relevant to the upcoming Phase III clinical trial.
- Results: The SCA can augment a reduced, real-world control arm to achieve desired statistical power, ensuring robust and ethical study design. Additional advantages of SCAs include exploring treatment combinations and extending observation periods by simulating control arms post-follow-up.
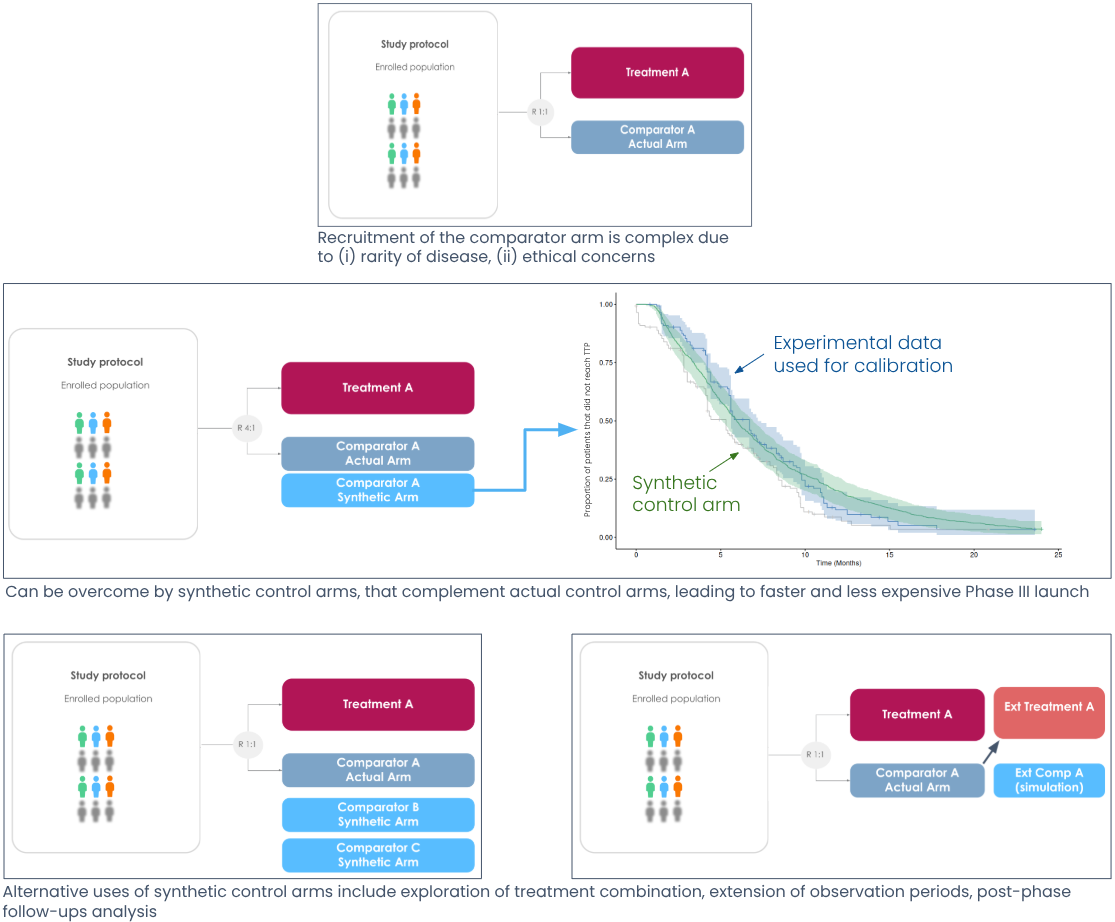
Overcome Phase III recruitment difficulties with synthetic control arms
EGFR-TKI treatments comparison - NSCLC
- Context: Clinicians needed comparative evidence on first- vs third-generation EGFR-TKIs in EGFR-mutated lung adenocarcinoma, yet running new head-to-head phase III trials is costly and slow.
- Methodology: An EGFR-driven NSCLC disease model, coupled with PBPK exposure models for gefitinib and osimertinib, was used to compute time-to-progression per RECIST 1.1 in an in silico head-to-head trial. The framework was calibrated to NEJ002/FLAURA data, its concordance confirmed via bootstrapped MaxCombo weighted log-rank tests, then applied to matched virtual cohorts to generate Kaplan–Meier curves and summary endpoints.
- Results: The framework reproduced mouse and human PK for both TKIs and recapitulated clinical TTP/PFS distributions with high concordance (e.g., ≥98% non-significant weighted log-rank comparisons in validation runs). It also anticipated the direction and magnitude of benefit in an external retrospective cohort (osimertinib > gefitinib) and enabled effect-model analyses to quantify patient-level benefit, illustrating how in silico trials can inform regimen selection without launching new phase III studies.
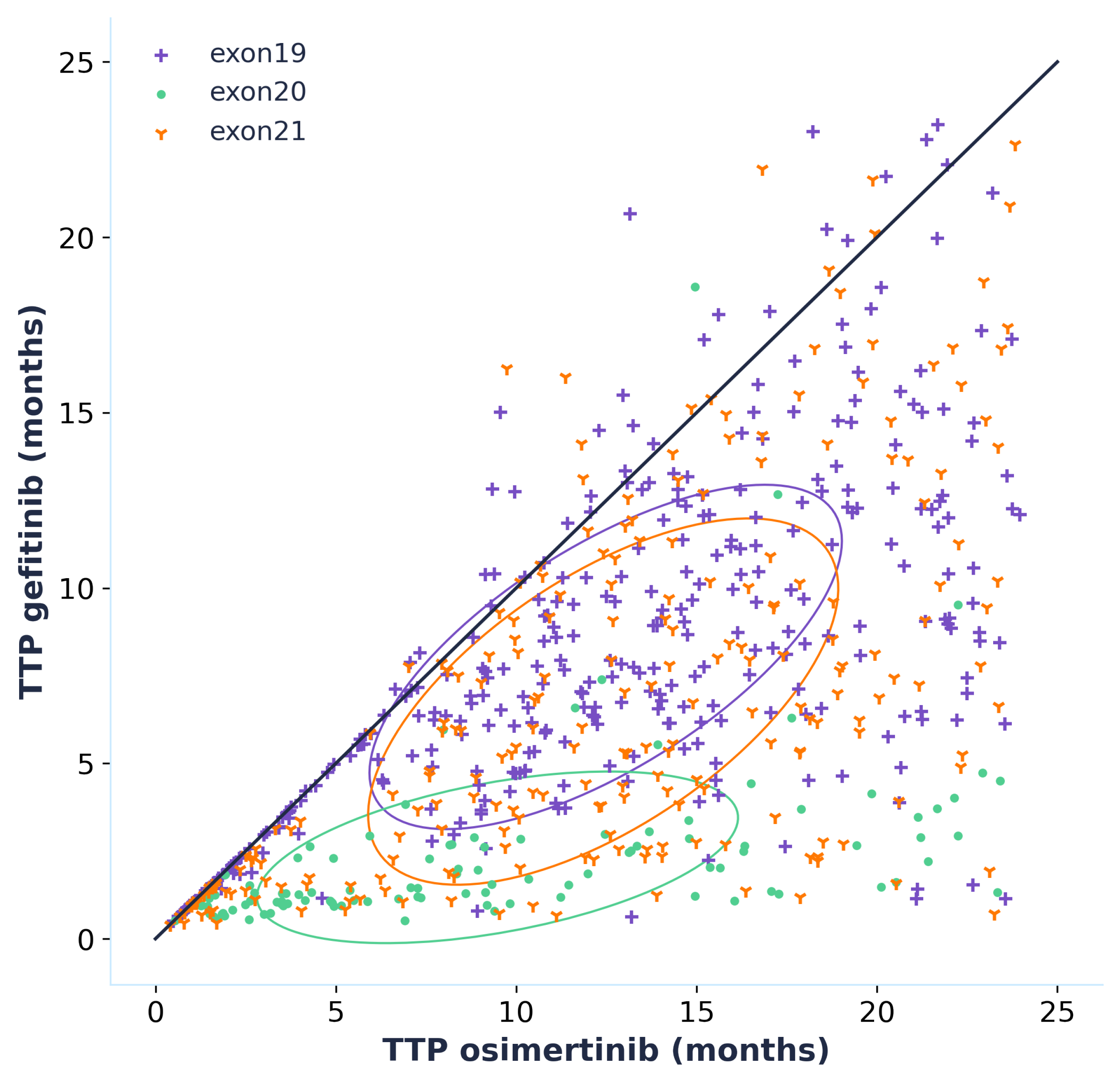
XY scatter plot comparing the effect of osimertinib and gefitinib in terms of time to progression (TTP) in a virtual population.
Each virtual patient is simulated twice (once with each treatment) and the population is stratify per EGFR mutations (exon 19, 20 and 21)
Treatment Combination - Chronic Hepatitis B (HBV)
- Context:
- A sponsor was developing a new treatment for chronic hepatitis B, with existing standards of care being inefficient.
- They had preclinical and Phase 1 data and hypothesized synergistic effects with combination therapies.
- The objective was to use mechanistic modeling to help the sponsor design the phase 2b trial, taking into account different possible combinations of the investigational dose and the existing SoCs, at different doses and schedules.
- Methodology:
- A computational model of chronic HBV patients was developed based on public and expert knowledge, non-clinical, and clinical data.
- The model was calibrated using published trial data and sponsor’s Phase 1 results.
- Simulations were run on a Virtual Population, testing more than 130 possible trial designs, changing the dose of each drug, the duration of treatment, all the different possible combinations, as well as different possible sequences in which the treatments would be administered.
- Testing all these scenarios in a real clinical setting would have required the enrollment of approximately 7000 patients, even assuming each arm would have only 50 patiens.
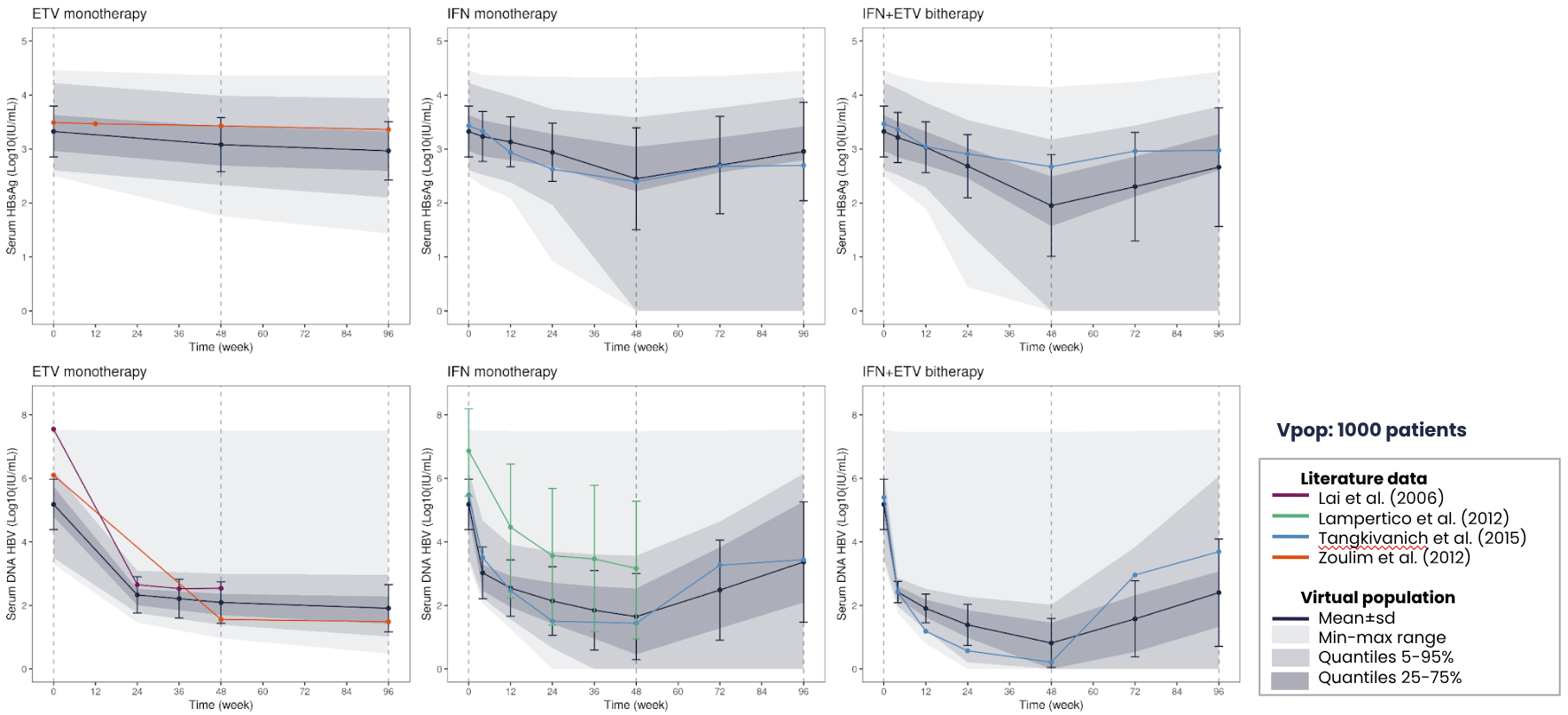
The model was calibrated to reproduce publicly available data for Entecavir (ETV) and pegylated interferon alpha (IFN).
- Results: Simulation results suggested that the sponsor’s treatment combined with PEG-IFNα2a was an optimal regimen, supporting selection of drug regimens for future Phase 2 trials (Granjeon-Noriot et al., 2021).
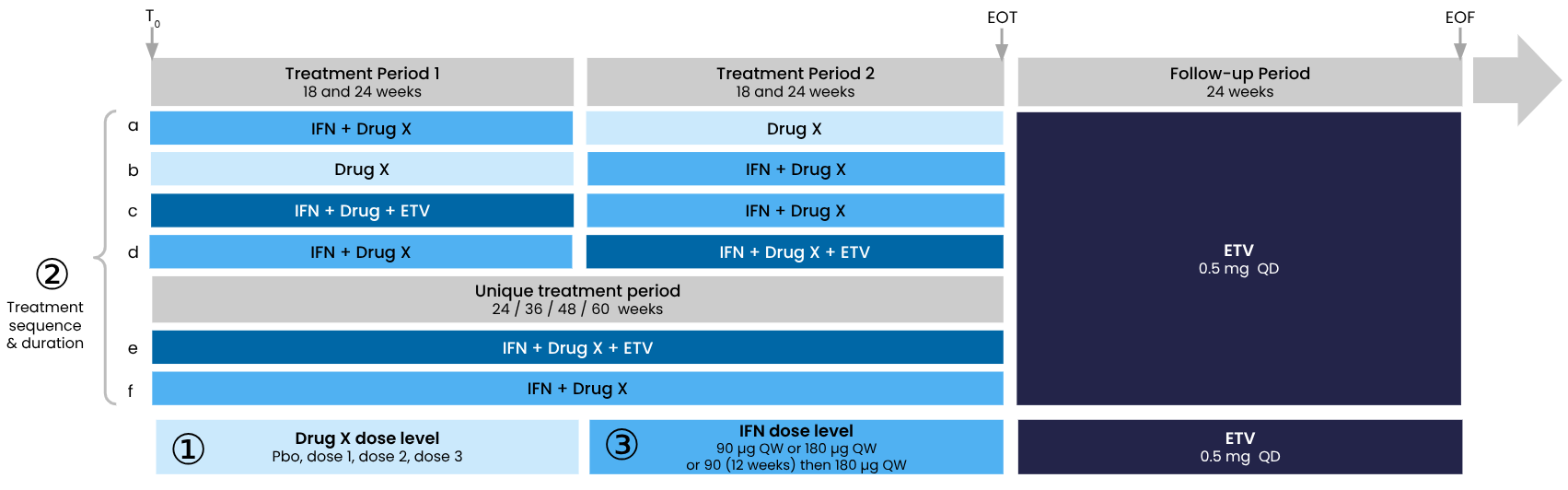
The model was used to simulate and compare the outcomes of different clinical trial designs, with several permutations of the combinations of treatments, dosage, treatment duration and treatment sequence.
Transposability Study - Population Extrapolation
- Context: Regulatory requirements in China and Europe necessitated new clinical data generation in both contexts, leading to a need to run minimal trials on selected subpopulations instead of all populations.
- Methodology: Two trials were run (one in China in adolescents, one in Europe in children). A QSP model, informed by these and historical trials, was used to generate missing data (e.g., efficacy in adults in Europe and China) to support label renewal. The methodology accounts for age and ethnicity-dependent variability in PK properties and disease progression.
- Results: The approach allowed for generating missing data to file for label renewal, demonstrating transposability across age groups and ethnic groups by accounting for physiological differences like immunosenescence and its impact on viral infections.
Trial Rescue/Monitoring - Subcutaneous to IV Administration
- Context: Observations of adverse effects with subcutaneous administration during a running Phase I trial necessitated a switch to IV administration for an upcoming Phase III trial.
- Methodology: An in silico drug-disease platform was developed and trained on the whole data package (preclinical to clinical). This platform was used to predict dose equivalence to switch to IV administration.
- Results: The model allowed for the translation of subcutaneous dose to an equivalent IV dose to avoid adverse effects, all while the trial was still running.
Treatment Regimen Optimization
- Context: A sponsor wanted to run a Phase 3 trial with an alternative regimen believed to be more efficacious than the classical regimen, and needed to convince regulators without including the comparison in the Phase 3 trial. They had heterogeneous Phase 3 adverse effects data.
- Methodology: An in silico trial was run to demonstrate the superiority of the alternative regimen over the classical regimen.
- Results: In silico results pointed to the alternative regimen being superior, with the effect increasing for shorter treatment durations.
Tangible Benefits of Digital Twins for Drug Developers
Better Trial Design & Success Rates
- Test unlimited trial designs on virtual patients to optimize protocols, identify best-responders, and maximize success odds.
- Systematically explore “what-if” scenarios in silico to reduce costly protocol amendments and late-stage failures.
- With pivotal oncology trials averaging $65mio per study and $100K per patient¹, even modest efficiency gains can prevent costly redesigns and late-phase failures.
Efficiency & Cost Savings
- Reduce required sample sizes and trial duration by supplementing or substituting control arms with credible digital twins.
- Compared to traditional methods, this can save years of development time and millions in costs: a ~4% increase in success probability translates into an additional $60mio in risk-adjusted NPV².
- Faster, leaner trials can reduce overall sample sizes, lower per-patient spend, and accelerate timelines by 3 to 9 months, directly cutting into the hundreds of millions invested in each Phase III program.
Patient-Centric Insights
- Capture rich patient heterogeneity to explore rare populations or biomarkers difficult to study in vivo.
- Optimize patient selection and address ethical concerns by minimizing exposure to ineffective treatments, while also reducing the number of patients who must be enrolled in costly pivotal trials.
- A shorter study duration (3–9 months faster to market) not only reduces direct spend but also secures earlier access to patent-protected revenues — for oncology assets, this can mean hundreds of millions in incremental revenue over the product lifecycle¹.
References:
- Clinical Trial Vanguard — 2022 Clinical Trial Budgets
- arXiv:2212.07384 — Assumed NPV of successful drug is US $1.62 bn
Tangible time and $ saved in recent projects
| Context | Value proposition | Outcome | ROI (company estimates) |
|---|---|---|---|
| Non-small cell lung cancer drug | Inform patient selection to capture best responders ahead of pivotal trial | 17% reduction in study sample size | $5M saved in study costs and 6 months saved in study duration translating into $765M in additional patent-protected revenues¹ |
| Non-small cell lung cancer drug | Explore treatment de-escalation scenarios to reduce side effects while maintaining drug efficacy | 20 simulated trials leading to one optimal treatment strategy | $76M saved in unnecessary parallel studies costs² |
| Atopic dermatitis drug | Inform patient selection to capture best responders ahead of pivotal trial | 25% reduction in study sample size | $5M saved in study costs 3 months saved in study duration translating into $125M in additional patent-protected revenues³ |
| Respiratory tract infections drug | Extrapolate drug efficacy from pediatric to adult patients | Label extension strategy informed by in silico study | $22M saved in avoidable study costs⁴ |
Footnotes
- Assuming lung cancer trial patient cost of $50K, initial sample size of 556 patients (clinicaltrials.gov) and on FY24 Tagrisso sales estimates of $1.5B (Global Data)
- Assuming 80 patients single study sample size
- Assuming $25K per patient variable costs, 800 patient pivotal study sample size (BMC Health Services Research) and FY24 median AD drug sales of $500M
- Assuming average pivotal study cost (adults) of $22M for an RTI drug (BMJ Open)
How we partner
Nova’s approach blends structured milestones with transparent and collaborative ways of working, ensuring both rapid proof points and long-term knowledge transfer.
Collaborative & Agile
- Weekly scientific meetings with partner teams.
- Agile and iterative process with next steps decided jointly.
- Early proof points (illustrative) ensuring quick wins within 2–3 months:
- Month 1: curated literature, model design validation, data foundation.
- Month 2: first running model, producing outputs for a reference patient.
- And steady progress toward major milestones.
- Month 3–4: Calibrated reference patient.
- Month 4–5: Calibrated virtual population.
- Month 6: First in silico trial readout.
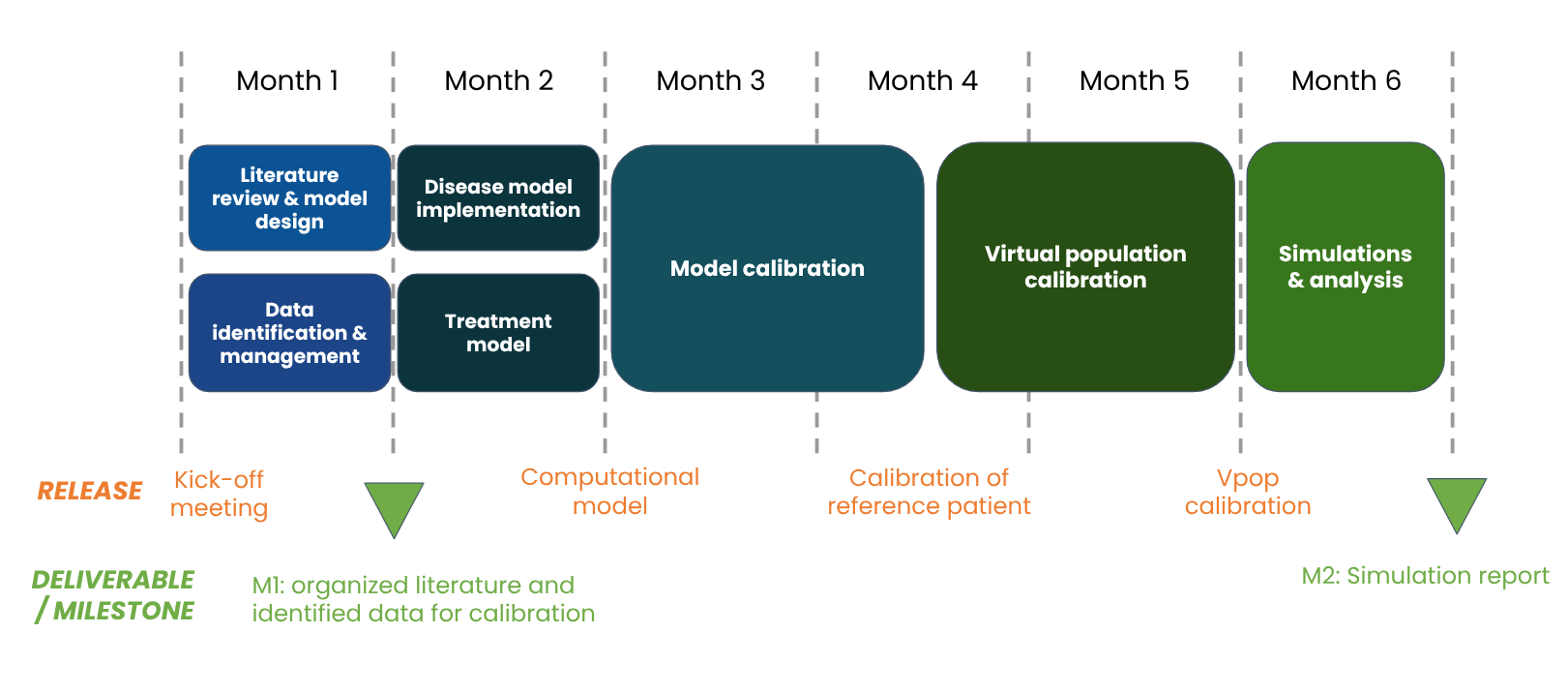
This timeline is illustrative, it might vary (~ +/- 1 month) as we iterate with partners over the scope of the model and its ultimate purpose.
Time savings: On average, 2 months saved for large projects when starting from an existing premium model from our model library.
Transparent & Auditable
- All knowledge, models, and data are organized in Jinkō and accessible to partners in a shared project space.
- Partners can audit, comment, and validate assumptions and outputs.
- Deliverables include documented calibration fits, scenario books, and simulation readouts, each fully traceable and reproducible.
Knowledge Transfer
- Partners are onboarded on Jinkō with a dedicated training program (~12 hours).
- Enables teams to:
- Edit their own models, trials, and protocols.
- Run their own experiments (within defined limits).
- Knowledge, assumptions, and results remain accessible after collaboration, ensuring continuity.
Unlimited Use & Licensing
- With a Jinkō subscription, partners can continue using the models and simulations beyond the initial project.
- Models can also be exported to other formats (SBML, Julia, …) for integration into internal platforms with a licence.
- Ensures sustainability of results and long-term scientific independence.
Nova In Silico: Company Description and Credentials
Nova In Silico is a pioneer in digital twin (DT) technology for clinical research, offering a proven platform that simulates patient outcomes with high fidelity. The company is driven by a long-term vision, enabling efficient and pragmatic engagement with sponsors.
Key Credentials and Capabilities:
-
Expert Team: Nova In Silico boasts a team of over 40 experts, including scientists, engineers, biologists, clinicians, and medical doctors. This multidisciplinary team works closely with sponsors from model conceptualization to simulation analysis, ensuring both scientific robustness and strategic insight. Their efforts are supported by a dedicated technical team of 20 numerical and optimization experts and data scientists continuously enhancing the Jinkō platform.
-
Extensive Model Library: The company has an extensive library of over 100 validated disease and treatment models across various therapeutic areas, including oncology (NSCLC, Hematology), cardiology, hepatology, infectious diseases, and rare diseases. This includes 12+ in-house trained/validated models and 80+ curated imports, providing a significant head-start for new projects.
-
Proven Track Record: Nova In Silico has delivered over 80 projects, demonstrating a strong track record of applying digital twins across therapeutic areas and clinical development phases. A landmark case includes accurately predicting the results of a Phase III lung cancer trial (FLAURA2) within hours, closely matching the real outcome.
-
Regulatory Alignment: Nova is at the forefront of regulatory science in the application of digital twin technology. While not a regulatory consulting firm, they actively support partners by delivering models and documentation that align with regulatory expectations. Jinkō’s white-box modeling approach provides full interpretability and traceability, well-suited for regulatory review. Submissions with QSP evidence to regulatory bodies like the FDA have shown increasing acceptance.
-
Collaborative Approach: Nova emphasizes a collaborative service model, involving partners’ clinical, digital, and statistical teams, as well as external experts, at every stage of model development. Scientific committees are embedded into their review cycles to ensure alignment with the current state of knowledge. Over 50 co-publications attest to their commitment to rigorous, collaborative science.
-
Proprietary Platform (Jinkō): Jinkō is Nova’s flagship enterprise-grade AI platform, purpose-built for biopharma. It integrates mechanistic disease modeling with AI/ML algorithms to create virtual patient “twins” and entire in silico cohorts. The platform supports the entire workflow from data ingestion to simulation output, offering features like knowledge management, virtual patient engine, mechanistic models, AI-powered calibration, and robust decision support.
-
Financial Stability: Nova In Silico is a profitable and privately owned company with no external investors at the board, indicating a stable and independent operational structure.