Atopic Dermatitis model
Model description
Nova’s atopic dermatitis (AD) model accounts for the interplay between the skin barrier and the immune system. It describes the key pathways and biomarkers influencing disease course, including the mechanisms driving the immune response dysregulation, the loss of skin barrier integrity and the perturbation of the skin microbiome.
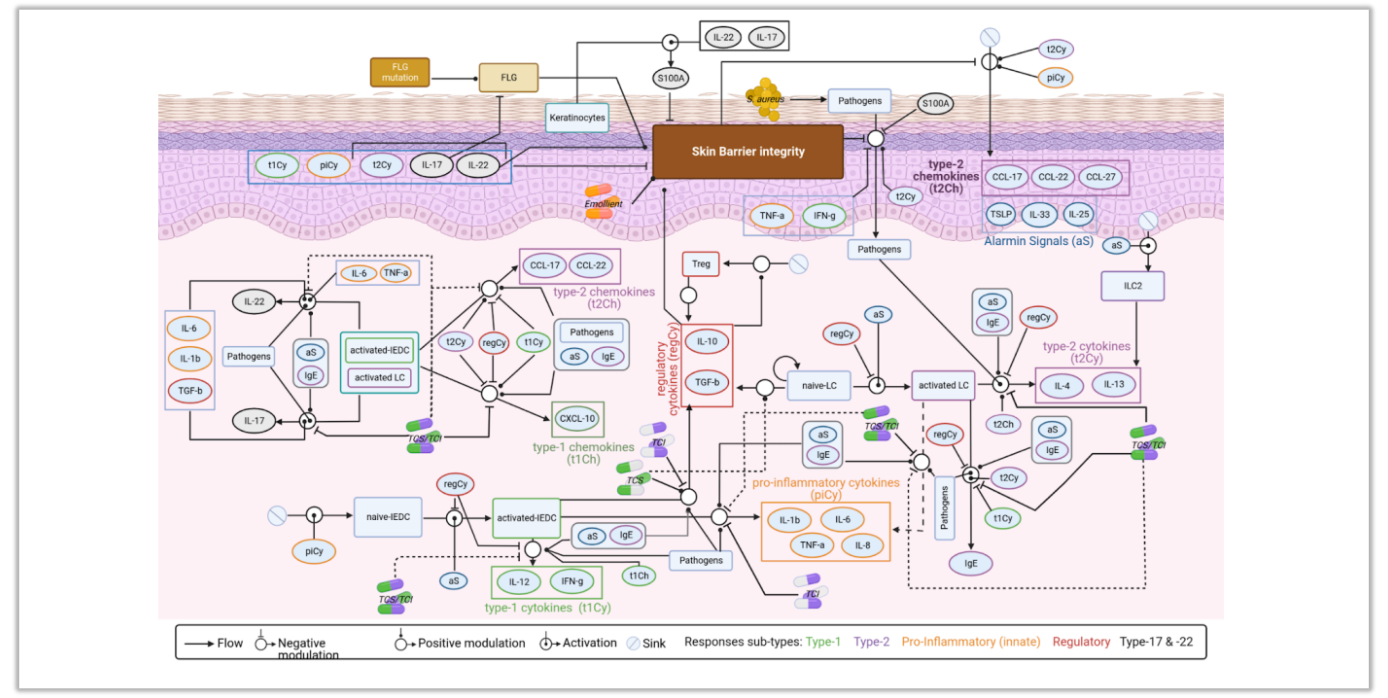
Atopic dermatitis (AD) model schematic. Exhaustive representation of the interplay between the skin barrier and the skin immune system (captured in the various immune responses subtypes) as well as mechanisms of actions of standard-of-care (SoC) treatments (topical corticosteroids (TCS) and emollients).
👥 Model Populations of interest
- Pediatric, adult population
- Mild, moderate or severe AD patients
- Specific AD endotypes (e.g. IL -17/11-22 high)
💊Drugs that can be tested
- Topical and systemic immunosuppressors (corticosteroids, NSAID)
- Other topical treatments (e.g. calcineurin inhibitors)
- Biologics (monoclonal antibody)
- More generally, topical or systemic investigational treatment
📍Possible clinical endpoints
- SCORAD/EASI
- Reduction in skin
- inflammatory biomarkers
Biological submodels
- Skin immune dysregulation
- Skin homeostasis (damage and repair)
- Standard of care treatments (emollients and topical corticosteroids)
Early insights to optimize your trial design - Atopic Dermatitis Model
Drug Regimen
- What is the impact of the dose per administration of an investigational treatment on pharmacodynamics markers?
- What is the impact of treatment duration?
- What is the best follow-up duration to assess efficacy?
Patient selection
-
What is the impact of selecting more (or less) severe patients?
-
What is the impact of selecting older patients?
-
Can better responder subtypes of AD can be identified? Based on which measurable biomarkers?
-
Can response be predicted based on a limited number of markers?
Combination of treatments
- What are the best combination of standard of care treatments (emollients, TCS) to include in both arms?
- What is the optimal TCS usage strategy?